Injection Instead of Laser May Be Viable Treatment Option for Diabetic Retinopathy
TEHRAN (Tasnim) – Among patients with proliferative diabetic retinopathy, treatment with an injection in the eye of the drug ranibizumab resulted in visual acuity that was not worse than panretinal photocoagulation at two years, according to a new study.
This study is being released to coincide with its presentation at the American Academy of Ophthalmology annual meeting.
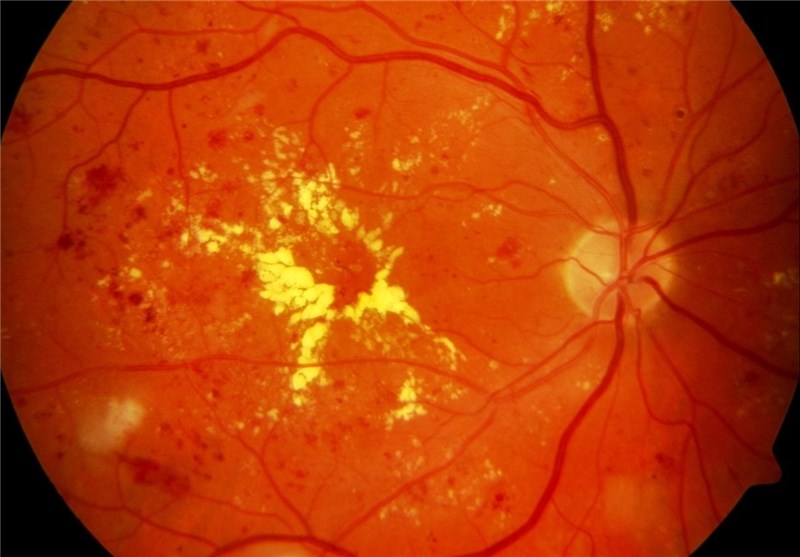
Proliferative diabetic retinopathy (PDR; a more advanced form of the disease) is a leading cause of vision loss in patients with diabetes mellitus, resulting in 12,000 to 24,000 new cases of blindness each year in the United States. Panretinal photocoagulation (PRP; procedure that involves use of a laser) is the standard treatment for reducing severe visual loss from PDR. However, PRP can cause permanent peripheral visual field loss and decreased night vision and may exacerbate diabetic macular edema (DME; swelling of the retina in diabetes mellitus due to leaking of fluid from blood vessels within the macula), which makes alternative treatments desirable, according to background information in the article.
When used as treatment of DME, intravitreous (in the vitreous, the fluid behind the lens in the eye) anti-vascular endothelial growth factor (VEGF) agents reduce the risk of diabetic retinopathy worsening and increase the chance of improvement, making these agents a potentially viable PDR treatment. Adam R. Glassman, M.S., of Jaeb Center for Health Research, Tampa, Fla., and the Writing Committee for the Diabetic Retinopathy Clinical Research Network, and colleagues conducted a study that included 305 adults with PDR; both eyes were enrolled for 89 participants (1 eye to each study group), with a total of 394 study eyes. Individual eyes were randomly assigned to receive PRP treatment, completed in 1 to 3 visits (n = 203 eyes), or the anti-VEGF agent ranibizumab, by intravitreous injection at study entry and as frequently as every 4 weeks based on a structured retreatment protocol (n = 191 eyes). Eyes in both treatment groups could receive ranibizumab for DME. The trial was conducted at 55 U.S. sites.
The researchers found that intravitreous ranibizumab met a prespecified noninferiority (not worse than) outcome of visual acuity change at 2 years than in the PRP group. There was no statistically significant visual acuity difference between the groups at 2 years, with the authors noting that 53 percent of the PRP group received ranibizumab injections for DME.
More peripheral visual field loss occurred, more vitrectomies (removal of the gel [vitreous] from within the eyeball) were performed, and DME development was more frequent in the PRP group compared with the ranibizumab group. No systemic safety concerns with ranibizumab were identified in the prespecified major safety outcomes.
"Although longer-term follow-up is needed, ranibizumab may be a reasonable treatment alternative at least through 2 years for patients with PDR," the authors write.
Editorial: Anti-VEGF Pharmacotherapy as an Alternative to Panretinal Laser Photocoagulation for Proliferative Diabetic Retinopathy
"In summary, this important study by the Diabetic Retinopathy Clinical Research [DRCR].net investigators represents a major step forward for patients with PDR by providing the ophthalmologists who manage their retinal disease with new options," writes Timothy W. Olsen, M.D., of Emory University, Atlanta, in an accompanying editorial.
"The short-term role (2 years) for using anti-VEGF agents seems to represent a viable alternative therapy for adherent patients with high-risk PDR. Nevertheless, PRP represents the standard of care for PDR and may represent the best long-term treatment option for high-risk PDR. It is certainly not time to abandon PRP in favor of exclusively treating patients with PDR using only intravitreal antiVEGF injections. Clinical judgment and timing of initiation of either therapy are viable options, and the findings reported by the DRCR.net researchers provide clinicians with evidence to support the alternative option of anti-VEGF pharmacotherapy for high-risk PDR. Further advances in pharmacologic management and sustained delivery systems will help expand this alternative therapy for PDR."





